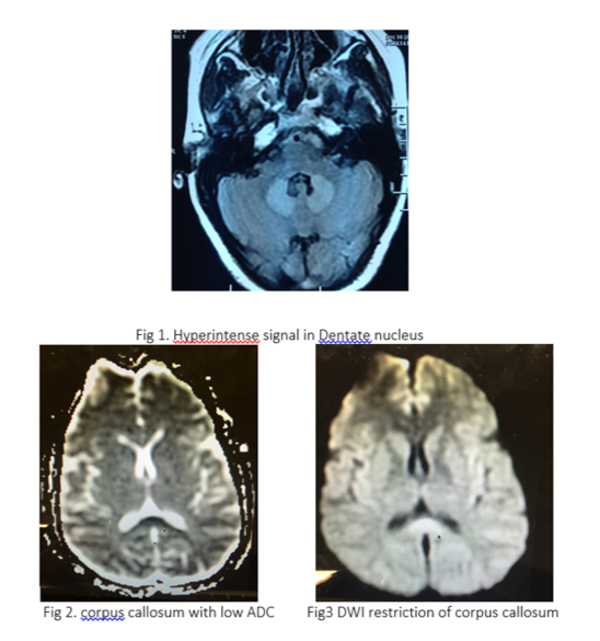
ABSTRACT Low Dose Metronidazole Induced Reversible Neurotoxicity Tina Ahluwalia Metronidazole is a well tolerated drug with limited side effects. Neurological presentation, due to its toxicity at doses as high as 34 grams have been reported in the past but never with low doses. Typical MRI findings show involvement of dentate nucleus and splenium of corpus callosum which are reversible within 3-8 weeks on stopping the drug. We report a case of acute onset pure motor UMN type of quadriparesis induced by low dose (8.4 grams total) Metronidazole treatment, given orally,with complete and early recovery, hastened by the use of parenteral steroids. Introduction: In1995 (1) Metronidazole induced cerebellar toxicity was identified, which reversed on discontinuation of this synthetic 5- nitroimidazole antibiotic. The exact cause of this is still debatable. MRI brain imaging suggest involvement of cerebellar nuclei and corpus callosum. With this case it’s evident that even lower doses of drug can induce toxic symptoms. Though the treatment involves discontinuation of the drug, we found that the recovery can be hastened with the use of parenteral steroid supporting the postulate that vasogenic oedema could be a cause of these cns symptoms. Case report: This 32 yrs lady was admitted for evaluation of acute onset, progressive symmetric quadriparesis since 5 days. She was apparently well 17 days ago when she developed gastroenteritis and was treated with Metronidazole tablets 400 mg tds for 7 days. Five days post treatment she developed ataxia, generalised weakness and diplopia on bilateral lateral gaze. There was no history of fever, rash, arthralgia, pain abdomen, headache, photophobia or bleeding from any site. There was no history of chronic illness in the patient and her family history was unremarkable. She is a vegetarian with nil addictions. Her daughter also suffered from gastroenteritis at the same time as her but recovered without treatment. Clinical examination revealed bilateral VI nerve palsy, UMN type of pure motor quadriparesis with power of 2/5 in all 4 limbs. Cerebellar signs, gait and rhomberg’s sign could not be assessed due to weakness and rest of the examination was unremarkable. A provisional diagnosis of cervical myelopathy vs ADEM was made and urgent MRI Brain with cervical spine was done which showed hyper intense signal in T2 and FLAIR images in the splenium of corpus callosum and dentate nucleus with diffusion restriction and low ADC (Fig 1-3) Cervical spine MRI was normal.
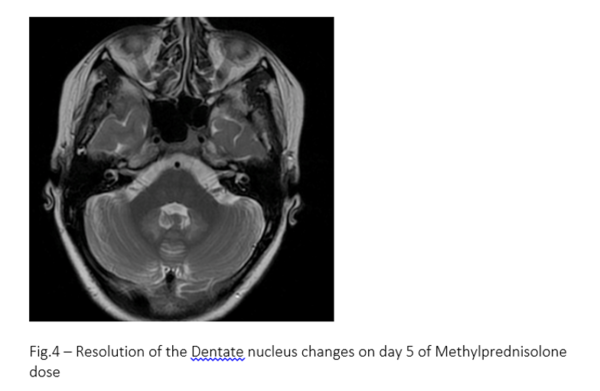
Lumbar puncture showed non-inflammatory results and oligoclonal bands were negative. Visual evoked responses and BAER were normal, ruling out demyelination as the possible aetiology. Patient was given Methylprednisolone 1 gm/day i/v for 5 days on which patient showed improvement and was able to stand by day 3. There was complete resolution of neurodeficit and cranial nerve palsy by the 5th day. A follow up scan showed a complete resolution of MRI changes (Fig4).
Discussion: Metronidazole induced encephalopathy (MIE) has been recognised as a rare toxicity which shares similarity with alcohol induced acute wernicke’s encephalopathy with the prominent cerebellar ataxia (2) and opthalmoparesis. In 1995 Ahmed et al (1) were the first to describe the involvement of cerebellum and correlated the findings with MRI picture of bilaterally symmetric lesions in cerebellar nuclei and corpus callosum. The Patho physiology behind MIE is still unclear, though some studies suggest metabolites of Metronidazole causing reversible axonal swelling by binding the RNA (3). Previous case reports have conflicting view regarding the correlation between dose and rout of administration of the drug. Some suggest that toxicities occur at a high total dose of 35gm over 30 days (1) and some studies found no correlation at all (4) however our case developed symptoms after 8.2 gms over 7 days. Mainstay of treatment of this neurotoxicity is drug discontinuation and supportive care . Evans J et.al (5) suggested diazepam could be used due to its GABA modulatory action as demonstrated in rats. We found that Methylprednisolone use resulted in early and complete recovery within 5 days. Conclusion: This case report introduces the idea that neurotoxicity with Metronidazole can occur at low doses which are commonly used in treatment of community acquired infections. Encephalopathy can even occur with oral preparation of Metronidazole and hence we recommend cautious use of the drug. The exact mechanism of the neurotoxicity remains debatable. Mainstay of treatment of this toxicity is stopping the drug however the use of Methylprednisolone can dramatically hasten complete clinical recovery. Referrals:
. |