ABSTRACT An Examination of Acute Medical Units in Scottish
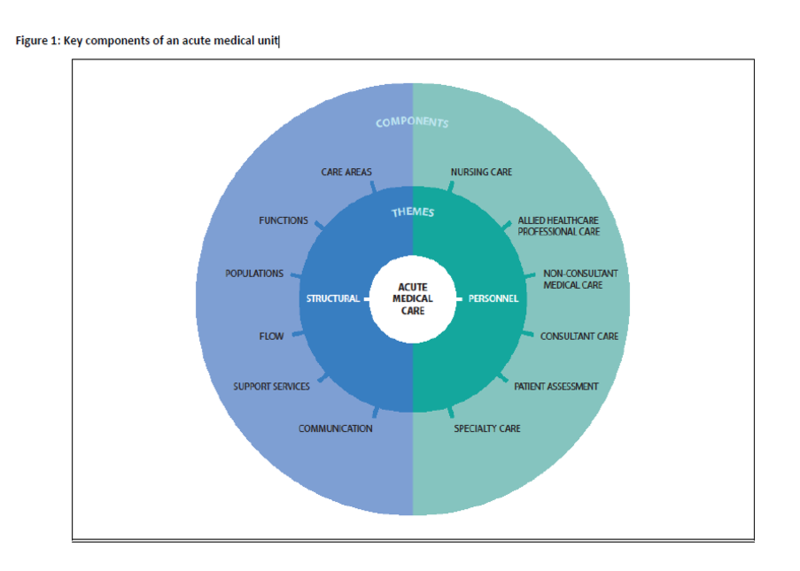
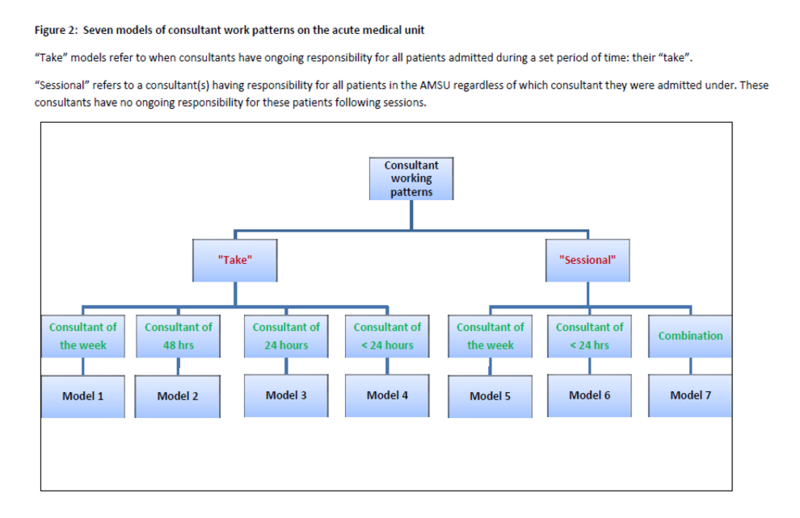
Hospitals Background and Aims: Acute medical units (AMUs) are the model of care for patients presenting with medical emergencies throughout the United Kingdom and Ireland, and are also present in Australasia and other European settings. AMUs emerged as a result of local service innovations and empirical evidence is lacking (1). We undertook a qualitative descriptive study to further examine the AMU model with the aim of informing service provision and contributing to the development of an evidence base relating to AMUs. Methods: All 29 AMUs in Scotland were studied. Data were collected through semi-structured interviews with a total of 275 health care professionals. These data were used to generate a report detailing how care was delivered in each AMU. These reports were then thematically analysed using framework analysis. Results: There were three principal findings. Firstly, we found that acute medical care was delivered in acute medical services comprised of multiple care areas rather than single AMUs. Secondly, we identified a framework of 12 key components of AMU care that were integral to the functioning of the AMU irrespective of the setting (Figure 1). Lastly, we described how these components were delivered across Scottish AMUs and, where possible, identified distinct models of care delivery. For example, we identified 13 models of AMU functions and seven models of consultant work patterns (Figure 2). In summary, we found that care in Scottish AMUs is delivered variably and there was little evidence of how best to deliver care. Conclusions: As the first in-depth study into AMUs, these findings provide a foundation for the onward planning of resources, capacity and standards of care at local, national and international levels. The finding of variation in care delivery is an impetus for further research to delineate how best to deliver care in AMUs. This study is an essential precursor to such work. References: 1Reid LEM, Dinesen LC, Jones MC, Morrison ZJ, Weir CJ and Lone NI. The effectiveness and variation of acute medical units: a systematic review. International Journal for Quality in Health Care, 2016, 28(4), 433–446
|